
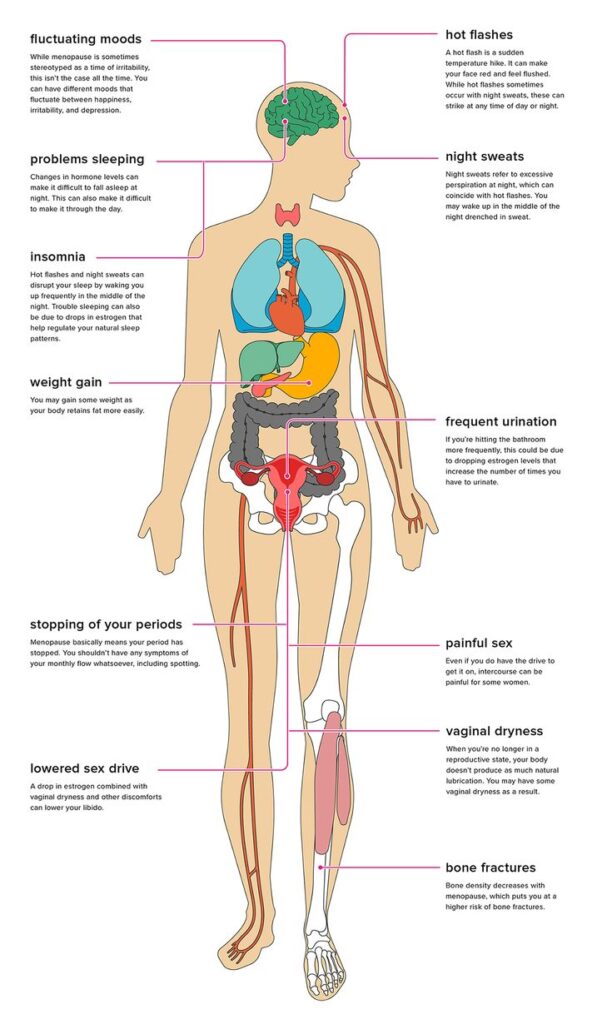
If you’ve wondered, “Could this be my hormones?” the short answer is often yes. During perimenopause (the transition years leading to menopause) and menopause (12 months without a period), estrogen and progesterone shift in ways that can affect nearly every system in your body. The graphic below highlights the most common symptoms—and why they’re real, common, and treatable.
What’s happening hormonally
- Estrogen fluctuates, then declines: Estradiol swings in perimenopause before trending lower in menopause. These changes influence temperature regulation, brain chemistry, sleep, vaginal tissue, bladder function, and bone remodeling.
- Progesterone drops earlier and more erratically: Lower, inconsistent progesterone can affect sleep, anxiety, and cycle patterns.
- It’s a network, not a single number: Hormones act like messages between organs. When signaling changes, effects show up head‑to‑toe.
How symptoms show up (and why)—head to toe
Brain fog and fluctuating moods
- Why: Estrogen modulates neurotransmitters (serotonin, dopamine) and blood flow. Swings can mean irritability, anxiety, low mood, and “where did my words go?” moments.
- What helps: Consistent sleep, daytime light exposure, strength training; for many, bioidentical estrogen plus bedtime progesterone; targeted non‑hormonal options when appropriate.
Sleep problems and insomnia
- Why: Night sweats wake you; lower progesterone can reduce the brain’s calming GABA activity.
- What helps: Cool, consistent routines; adjust caffeine/alcohol timing; oral micronized progesterone at night for many; address vasomotor symptoms (often with estrogen).
Hot flashes and night sweats
- Why: Estrogen influences your hypothalamic “thermostat.” As levels change, the comfort zone narrows, triggering heat waves and sweating.
- What helps: Transdermal bioidentical estrogen is first‑line for many; non‑hormonal options exist (certain SSRIs/SNRIs, gabapentin). Cooling strategies help while treatment takes effect.
Sleep problems and insomnia
- Why: Night sweats wake you; lower progesterone can reduce the brain’s calming GABA activity.
- What helps: Cool, consistent routines; adjust caffeine/alcohol timing; oral micronized progesterone at night for many; address vasomotor symptoms (often with estrogen).
Weight gain and body composition shifts
- Why: Estrogen changes can affect insulin sensitivity and fat distribution (more midsection). Sleep loss and stress compound the effect.
- What helps: Progressive strength training 2–4x/week, protein targets, walking, metabolic labs (glucose, insulin, lipids). Hormone therapy can support sleep and energy—the foundation for sustainable change.
Low libido and painful sex
- Why: Lower estrogen reduces vaginal blood flow and lubrication; tissues thin and become less elastic (genitourinary syndrome of menopause). Desire dips when sleep and mood suffer.
- What helps: Local vaginal estrogen (very low systemic exposure) is highly effective. Systemic therapy may help libido indirectly via sleep/mood; carefully dosed testosterone may be considered in select cases. Pelvic PT can be game‑changing.
Vaginal dryness and urinary urgency
- Why: The vagina, urethra, and bladder are estrogen‑sensitive; lower estrogen leads to dryness, discomfort, urgency, and recurrent UTIs.
- What helps: Local vaginal estrogen or DHEA, quality moisturizers/lubricants, pelvic floor physical therapy, hydration and bladder training strategies.
Period changes and menopause
- Why: Ovarian hormone production declines; cycles become irregular, then stop. Menopause is 12 months without bleeding (not caused by another condition).
- What helps: If you have new bleeding after 12 months period‑free, get evaluated—don’t ignore it.
Bone density and joint aches
- Why: Estrogen supports bone remodeling; lower levels accelerate bone loss. Some notice new joint stiffness or aches.
- What helps: Strength training, adequate protein, vitamin D/calcium as appropriate, fall‑prevention strategies, and considering systemic estrogen near menopause for bone protection if you’re a candidate. A DEXA scan may be recommended.
The “surprising symptoms” you might not connect to hormones
Palpitations, headaches, dry eyes/skin, tinnitus, and bladder changes can all be part of the hormone story. You’re not imagining it—and you’re not alone.
What a practical plan can include
- Listen first: Your symptoms lead; labs guide. We don’t let a “normal” result override how you feel.
- Smart testing: In‑office fasting labs (thyroid, metabolic markers) to personalize and keep care safe. Sex‑hormone testing is used when it changes a decision or fine‑tunes therapy.
- Evidence‑based hormone therapy: Bioidentical estrogen and progesterone (and when appropriate testosterone) using adjustable forms—not pellets—plus local vaginal estrogen when needed.
- Regular follow‑ups: Early check‑ins (about every six weeks) to adjust dose/route and track progress.
- Lifestyle that compounds results: Sleep strategies, strength training, protein targets, stress tools, and pelvic PT when helpful.
Perimenopause and menopause can touch every part of life—sleep, mood, focus, intimacy, energy, confidence. These symptoms are common and real, and there are safe, evidence‑based ways to feel better. You don’t have to accept “it’s just aging.”


